
CO-119 Denial Code Description: Benefit Maximum Reached in DME
July 14, 2026
What is revenue cycle management in DME? It is the end-to-end process of tracking a piece of equipment from order to payment, and in DME it lives or dies on documentation. The complex rule load is what sets it apart from standard healthcare billing, and it is why so much revenue leaks at the very start of the cycle: intake.
What is DME Revenue Cycle Management?
What is revenue cycle management for DME suppliers? It is the specialized process providers use to track, manage, and collect revenue for physical equipment.
This medical revenue cycle management lifecycle bridges the gap between delivering items and securing reimbursement through six strict stages:
- Intake and Eligibility: Staff collect patient demographics, verify insurance coverage, and determine pre-authorization requirements.
- Documentation and SWO: Providers secure a compliant Standard Written Order (SWO) and clinical notes to prove medical necessity prior to delivery.
- Coding: Clinical documentation and diagnoses are translated into standardized HCPCS, ICD-10, and CPT codes required by payers.
- Claim Submission: The coded claim is scrubbed for errors and submitted to the insurance provider.
- Denial and Appeal: If a payer rejects the claim, the team investigates the error, corrects it, and submits a formal appeal.
- Payment: The cycle concludes when the insurer issues payment, the provider posts the remittance, and any remaining balance is handled per the patient’s plan.
How DME RCM Differs from Standard Healthcare RCM
What is revenue cycle management when applied to equipment instead of physician services? It is a fundamentally different process because DME manages physical products, making claims heavily reliant on strict documentation and specific payer logic.
Coding and Billing Logic
To understand revenue cycle management in DME, you must recognize how coding and billing logic dictate the reimbursement process.
Standard RCM uses CPT codes for procedures. DME relies on HCPCS Level II codes, such as E codes for equipment and A codes for supplies, combined with specific modifiers.
- Rental vs. Purchase: Standard healthcare bills once for a service. DME involves capped rentals paid in monthly installments for up to thirteen months until ownership transfers, or continuous payments for up to thirty-six months.
- Same-or-Similar Equipment: Before providing an item, staff must run checks to verify the patient has not recently received the same or similar equipment to avoid duplicate claim denials.

Clinical and Delivery Requirements
When evaluating revenue cycle management for equipment, you must account for the strict clinical and delivery requirements that standard billing ignores. DME requires absolute adherence to specific coverage and delivery criteria that physician services do not.
- Face-to-Face (F2F): Items on CMS’s Required Face-to-Face and Written Order Prior to Delivery (WOPD) list require a practitioner encounter within the six months preceding the order, with the written order completed and on file before delivery.
- LCD/NCD Compliance: DME requires strict adherence to region-specific Local Coverage Determinations (LCDs) and National Coverage Determinations (NCDs) that dictate exact ICD-10 codes and testing criteria for coverage.
- Proof of Delivery (POD): DME requires undeniable Proof of Delivery, including a patient or caregiver signature and date, matching the exact date of service on the claim. Without it, payers recoup funds or deny the claim.
Where Revenue Leaks (And The Documentation Layer That Stops It)
Where is a DME revenue cycle most vulnerable? Revenue leaks primarily stem from front-end intake and documentation failures, triggering costly claim denials and delays.
Top Revenue Leaks in DME
Revenue leaks usually happen when documentation fails to prove medical necessity. Revenue leaks in DME occur when compliance gaps trigger rework and accounts receivable delays.
- Incomplete Intake and Medical Necessity Documentation: Every DME claim requires extensive documentation based on payer-specific LCDs and NCDs. If the SWO lacks details or face-to-face encounter notes are unsigned, payers reject the claim.
- Manual Data Entry Errors: Extracting patient demographics and physician details from unstructured medical records manually invites human error. A single wrong modifier or mistyped NPI turns a clean claim into a denied one.
- Delayed Corrections and Addendums: When a payer flags incomplete clinical notes, providers face long back-and-forths with prescribing physicians. This delay pushes accounts receivable cycles beyond one hundred twenty days, reducing the chances of recovering the billed amount.

The Documentation Layer that Stops Leaks
Most of these leaks start in the same place: intake. A billing team or an outsourced RCM partner can chase the denial after the fact, but neither fixes the root cause, which is documentation that was incomplete before the claim was ever built. That is a front-end problem, and it needs a front-end fix.
CompliantRx was built by a DME operator to work at that front end. It is not an RCM or billing platform; it is the intake and compliance layer that sits ahead of your revenue cycle and makes sure the record is complete and compliant before a claim goes out. Clean intake is what a healthy revenue cycle is built on.
Here is how it works at intake:
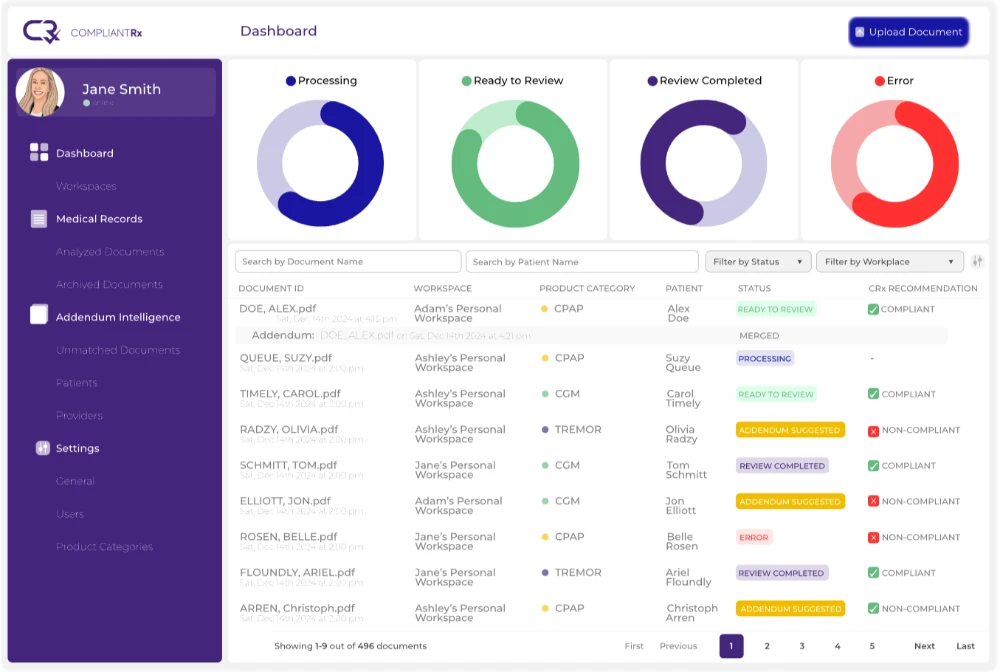
- AI Medical Record Review scans incoming documentation against Medicare and payer-specific rules and flags anything missing before a claim is built.
- Intelligent Data Extraction pulls patient and physician details from faxes and referrals, reducing manual data entry.
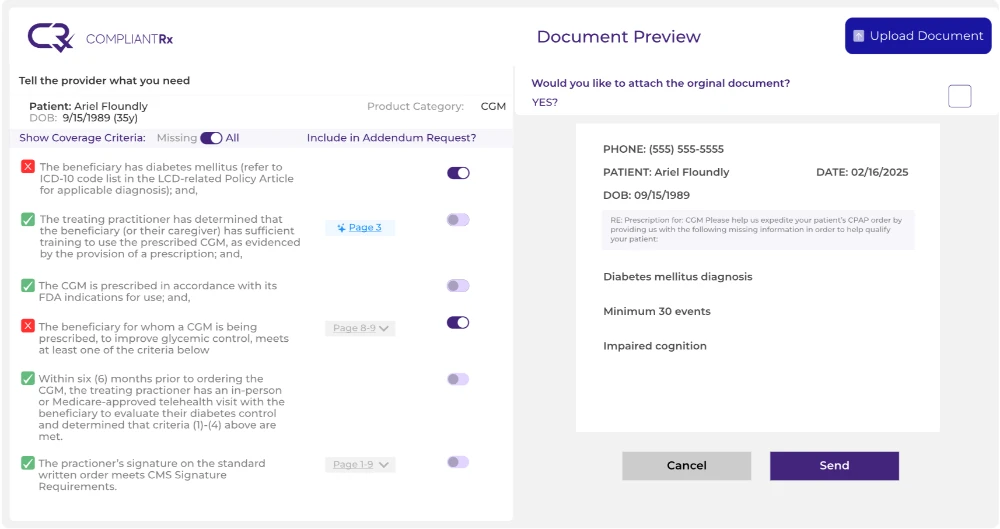
- Addendum Intelligence™ auto-generates the corrective addendum to send back to the provider for anything incomplete.
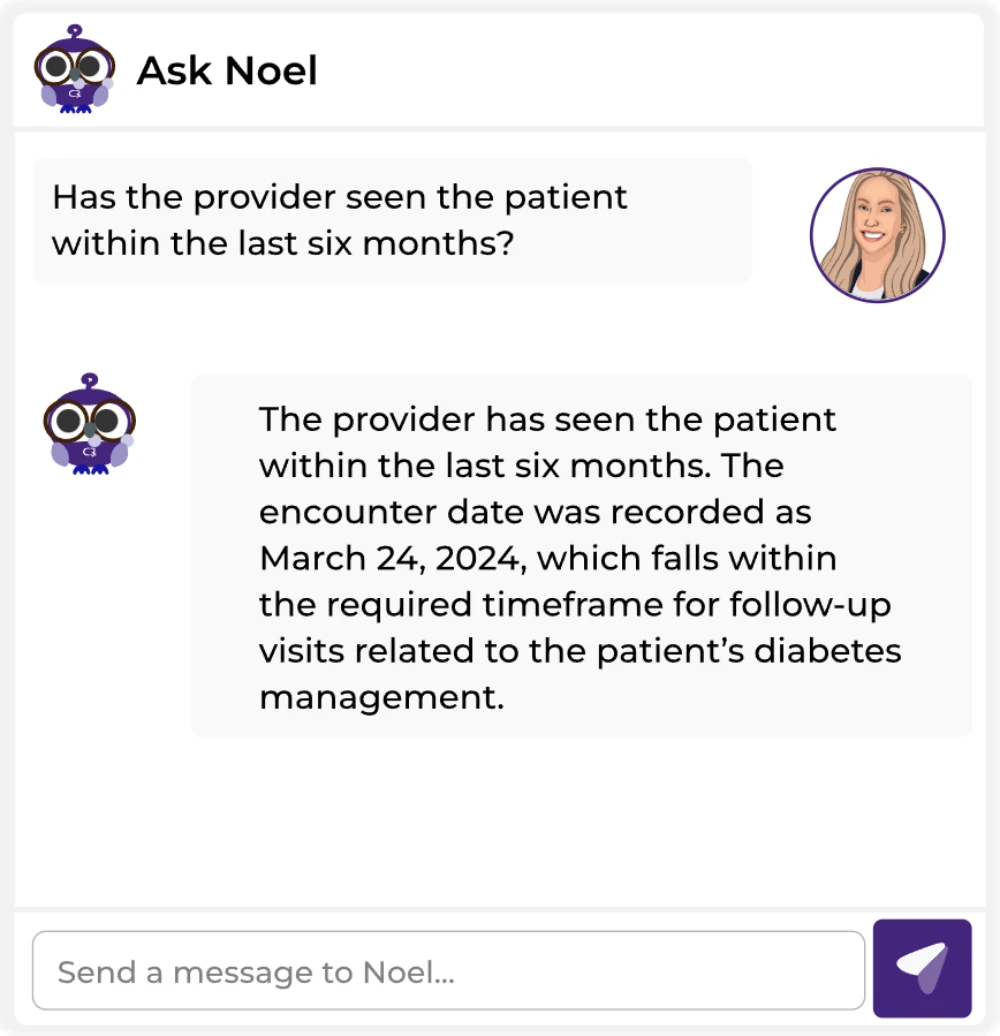
- Ask Noel® gives your team product-specific compliance answers, so they know what documentation is required upfront.
Key Takeaways: Build a Compliant DME Revenue Cycle
DME revenue cycles suffer when documentation fails to meet strict payer rules and product-specific requirements. Understanding “what is revenue cycle management” in this space means recognizing that a clean revenue cycle starts with clean intake.
CompliantRx works at that first step, catching documentation gaps before claims go out, so fewer denials reach your revenue cycle in the first place. Schedule a demo to see how it fits your intake workflow.
FAQs
Here are common questions providers ask when evaluating “what is revenue cycle management” for their DME operations.
1. How do capped rental rules affect cash flow?
Capped rental items require monthly billing over thirteen months before ownership transfers, which delays full reimbursement compared to retail sales. Managing these installments requires careful tracking to ensure continuous payment collection.
2. What triggers an audit for a DME supplier?
Audits are typically triggered by billing patterns that deviate from peers, high volumes of specific high-cost items, or missing documentation. Maintaining complete clinical records before submission remains the best defense against these reviews.
3. Why do same-or-similar denials occur frequently?
These denials happen when a patient receives equipment that duplicates an item recently provided. Checking the patient claim history prior to delivery prevents these costly duplicate submissions.
4. How does CompliantRx integrate with existing ERPs?
CompliantRx connects with systems of record like Brightree and NikoHealth without an IT overhaul, so your staff keep their current workflow while adding an automated compliance check at intake.



{kind=link}
{kind=link}
{kind=link}