
Denial Management in Medical Billing: A DME Supplier’s Guide
July 13, 2026
A PR-204 denial code description states that the service, equipment, or drug is not covered under the patient’s current benefit plan, with the PR group code marking it patient responsibility.
For DME suppliers, it usually means the equipment is excluded, blocked as same-or-similar, or not covered at delivery. Here is how to read and prevent it.
What Does PR-204 Mean?
The PR-204 denial code description starts with the X12 CARC definition and the group code that precedes it. The code surfaces after adjudication, confirming the claim reached the payer and failed coverage policy rather than bouncing for a formatting error.
The Official Descriptor
CARC 204 carries the official descriptor: “This service/equipment/drug is not covered under the patient’s current benefit plan.” Noridian, the DME MAC administrator, often pairs it with remark code N130, which directs providers to consult plan benefit documents for service restrictions.

The PR group code stands for Patient Responsibility, signaling the amount may be billable to the patient when plan language and notice rules permit. That differs from a CO-204 denial code, where the CO (Contractual Obligation) group code means the provider absorbs the cost instead of billing the patient.
This code surfaces post-adjudication, meaning the payer accepted and processed the claim. The denial reflects a coverage decision based on plan design, not a submission error.
Key Details and Billing Context
First, the payer processed the claim and applied a coverage adjustment, so formatting and routing were valid.
Second, N130 often accompanies 204 on DME remittances, pointing you to plan documents and the governing LCD or NCD.
Third, Noridian lists non-covered or not-medically-necessary items as standard reasons, often tied to same-or-similar history or frequency limits.
Why PR-204 Hits DME Claims
The PR-204 denial code description maps to four recurring DME scenarios that shift financial liability to the patient. Each situation is preventable when coverage and equipment history are verified before the item ships.
Equipment Not Covered
The item may be excluded from the plan or fall outside Medicare’s statutory definition of DME. To be covered by a DME MAC, an item must fall within a Medicare DME benefit category.
Items that do not, or are statutorily excluded, produce a 204 denial. Upgrades such as smart beds and experimental devices are common examples.
Same-or-Similar Restrictions
Payers track capped rental and lifetime use. If a patient already uses a same-or-similar item, or the prior rental period has not closed, a new claim for the same device denies.
Noridian’s Same or Similar Chart helps suppliers check history before delivery. Suppliers must query the patient about existing equipment and check payer history files before processing the order.

Frequency Caps
Medicare’s reasonable useful lifetime for most DME is no less than five years, counted from the delivery date. CPAP masks and tubing typically replace every three months, with items like chin straps every six months.
Billing before these intervals elapse triggers a 204 adjustment. Suppliers must track replacement schedules meticulously.
Eligibility Lapse Between Referral and Delivery
Coverage is evaluated on the Date of Service, which for DME is usually the delivery date. If a prior authorization is approved but coverage terminates before the equipment is delivered and signed for, the claim denies as non-covered. You must re-verify eligibility on the exact date of delivery, not just the date the order was initiated.
What To Do When You Get One
Once you understand the denial, your response depends on the root cause behind the adjustment. The steps below cover the most common next steps for resolving this denial.
- Receive PR-204 denial -> Review the EOB and identify the root cause.
- Coding or plan error -> Verify HCPCS or CPT codes and the billed payer -> Correct and resubmit the claim.
- Covered and necessary item -> Gather clinical notes and a letter of medical necessity -> File a redetermination through the payer portal within 90 to 180 days.
- Strict plan exclusion -> Confirm plan exclusion language, network status, and ABN or No Surprises Act rules -> Bill the patient or process a write-off.
- Repeat denials -> Implement front-end eligibility checks and prior authorization tracking -> Prevent future PR-204 adjustments.
If you decide to appeal, Noridian encourages filing through the Noridian Medicare Portal after reviewing the LCD and documentation checklists.
If the plan strictly excludes the service, the amount may shift to the patient, but only when allowed.
The PR group code signals potential liability, not automatic billing authority. You must confirm plan exclusion language, network status, and ABN or No Surprises Act rules first.
Preventing PR-204 in DME
PR-204 points to a front-end problem, which is why prevention beats appeal. CompliantRx was built by a DME operator to check coverage rules, clinical documentation, and prior authorization at intake, before a non-covered item ever reaches the payer.
Real-Time Eligibility and Benefit Checks
Our platform validates which codes are covered under the patient’s active policy before submission, flagging excluded items at intake. This helps keep non-covered equipment out of the billing queue.
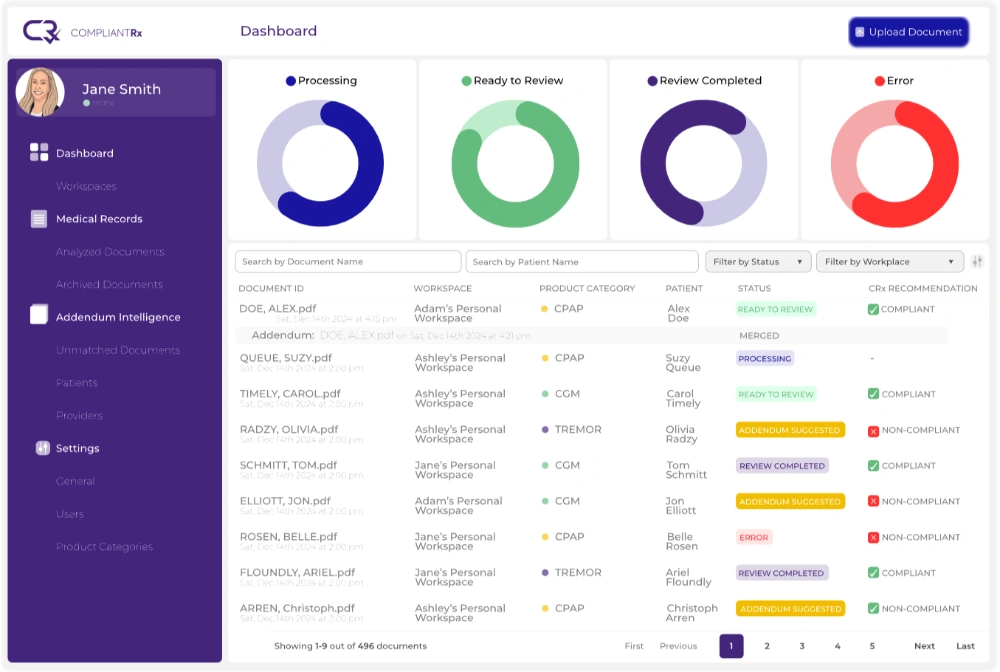
AI-Powered Documentation Auditing
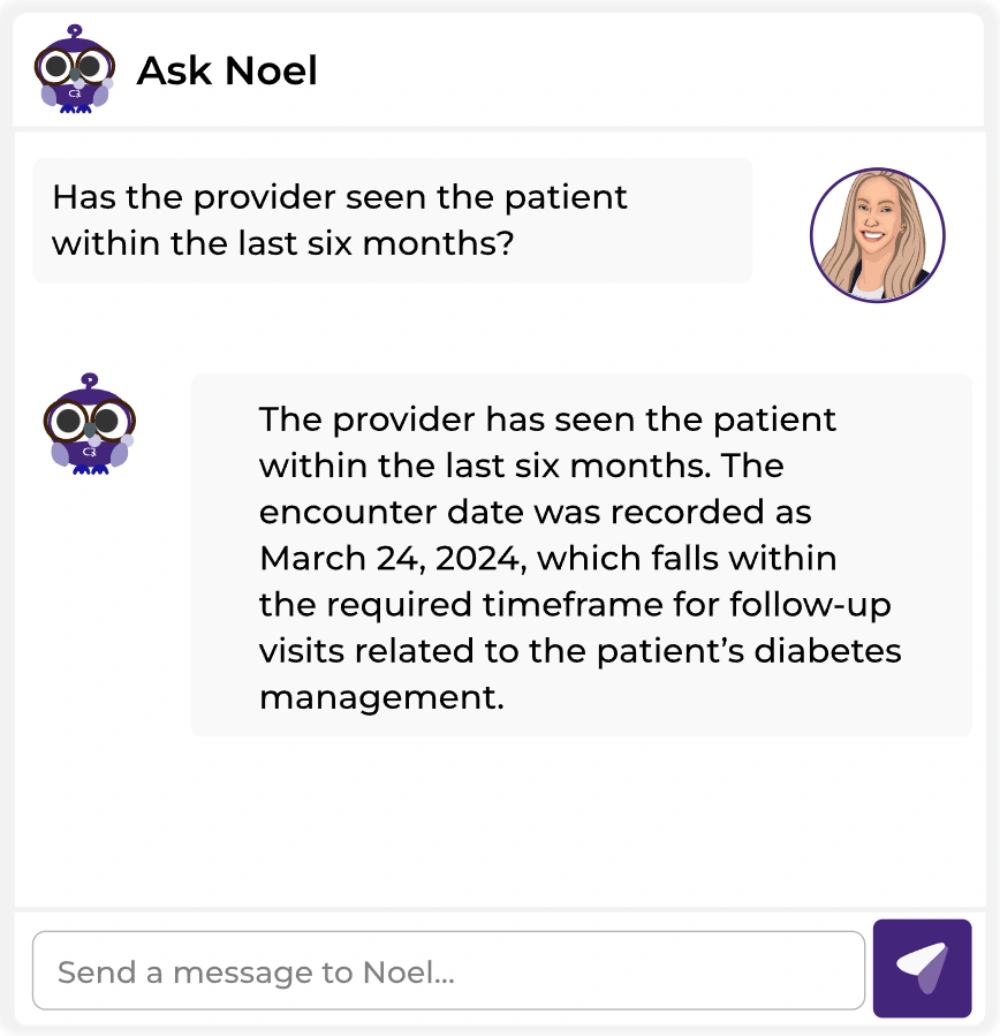
AI Medical Record Review scans incoming faxes and notes against the applicable rules to confirm the documentation supports medical necessity. Ask Noel® delivers product-specific compliance answers to guide your intake staff through complex payer rules.
Pre-Authorization Management
CompliantRx identifies services requiring prior authorization and tracks approval numbers to help prevent rejections from missing or expired authorizations.
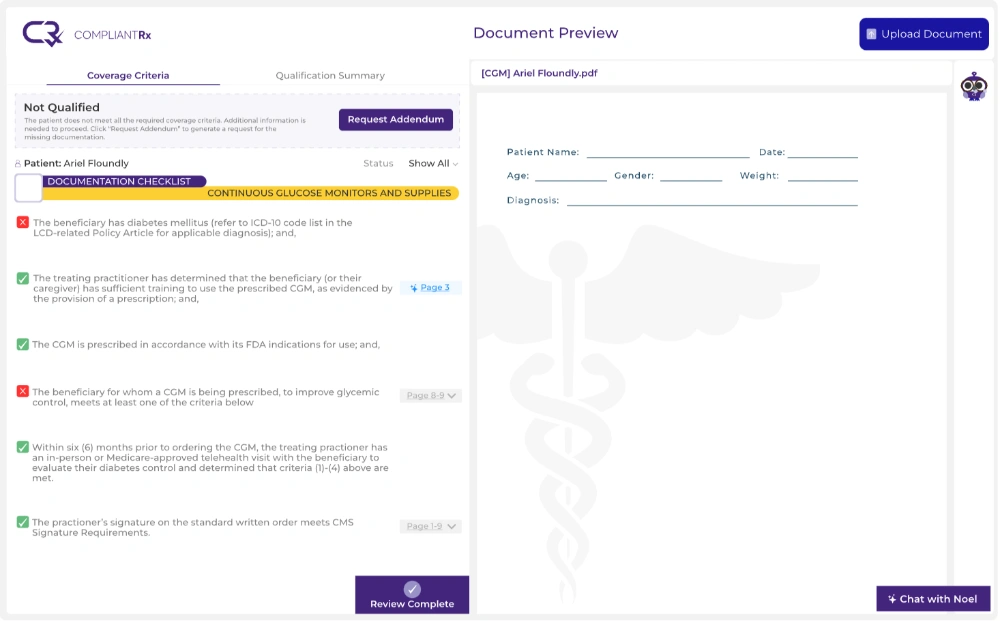
Automated Coverage Rules
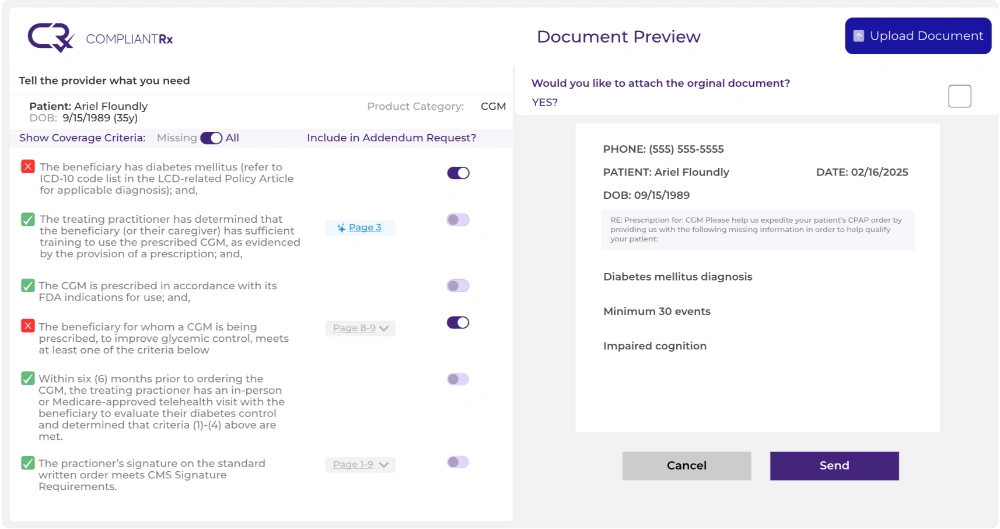
The platform cross-checks items against payer-specific LCD and NCD guidelines. Addendum Intelligence™ generates payer-compliant addendum requests when gaps appear, and Intelligent Data Extraction pulls patient and physician details from records. It connects with systems of record like Brightree and NikoHealth, with HIPAA-compliant data handling and audit trails.
Key Takeaways: Make PR-204 a Front-End Catch
The PR-204 denial code description comes down to one issue: the equipment is not a covered benefit, often due to same-or-similar conflicts, LCD criteria, or coverage lapsing between referral and delivery.
The fix is front-end verification of coverage and equipment history before the item ships. Schedule a demo to see how CompliantRx flags non-covered items at intake.
FAQs
1. Is PR-204 the same as the PR204 denial code?
Yes, the PR204 denial code is the no-hyphen shorthand for PR-204, pairing the Patient Responsibility group code with CARC 204. Both indicate a service not covered under the patient’s current benefit plan.
2. Does PR-204 mean my claim was rejected for a typo?
No, the code appears after adjudication, meaning the payer accepted and processed the claim. It reflects a coverage decision based on plan design, not a formatting or routing error.
3. Can I always bill the patient after a PR-204?
No, the PR group code signals potential patient liability, not automatic billing authority. Whether you can bill depends on plan exclusion language, network status, and ABN or No Surprises Act rules.
4. Can CompliantRx check same-or-similar history before delivery?
Yes, our platform cross-checks submitted items against payer coverage rules and LCD criteria at intake. This helps flag same-or-similar conflicts before the equipment ships.



{kind=link}
{kind=link}
{kind=link}