
What Is DME Compliance? How to Build a Program That Actually Works in 2026
May 26, 2026
Denial Management in Medical Billing: A DME Supplier’s Guide
July 13, 2026
The most frequent common denial in medical billing for DME suppliers traces back to one place: intake. Eligibility gaps, missing prior authorizations, and documentation errors almost always start when the order first comes in and gets reviewed by hand.
Catch these eight rejection categories at intake, before the claim ever reaches the payer, and you protect both your cash flow and your team’s time.
The Most Common Denial In Medical Billing Categories For DME
We outline the eight primary rejection categories and provide a one-line fix for each to help you secure reimbursement.
1. Eligibility and Coverage Errors (incl. PR-204)
PR-204 denials occur when the billed item or service is explicitly excluded from the patient’s current insurance policy or benefit plan.
The prefix “PR” indicates patient responsibility, meaning the patient will likely be billed out-of-pocket unless an alternate payer or secondary insurance exists. This frequently happens with statutorily non-covered items, out-of-network providers, or lifetime benefit caps.
Prevention: Verify comprehensive insurance eligibility, plan benefits, and coverage rules in real time prior to delivering any equipment, and obtain a signed ABN (Advance Beneficiary Notice) where the payer’s rules allow it.
2. Prior Authorization Gaps
Prior authorization (PA) denials happen when suppliers fail to get formal pre-approval from the payer before delivering high-value DME. Payers require this to ensure the equipment meets medical necessity guidelines before it reaches the patient. Forgetting this step typically results in an automatic rejection.
Prevention: Always confirm PA requirements via the Medicare Coverage Database and secure authorization codes before shipping items, ensuring approval is documented before the date of service.
3. Documentation and Medical Necessity Failures
These denials occur when clinical records fail to substantiate medical necessity. Triggers include missing Standard Written Orders (SWOs), invalid Face-to-Face (F2F) encounters, or absent Proof of Delivery (POD).
These gaps typically surface as CO-16 denials (claim/service lacks information needed for adjudication, always paired with a remark code identifying the missing element) or, after clinical review, as CO-50 medical-necessity denials.
Prevention: Utilize digital checklists to ensure SWOs and F2F notes are perfectly executed before delivery, and track CMS Standard Documentation Requirements to maintain compliant proof of delivery.
4. HCPCS and Modifier Mismatches
These denials arise when the submitted HCPCS code misrepresents the equipment or when vital modifiers are mismatched, outdated, or completely omitted. Modifiers provide critical context, like indicating whether equipment is new (NU), rented (RR), or purchased (UE). Missing or invalid combinations make claims unprocessable.

Prevention: Train billing staff to cross-reference equipment with CMS HCPCS Level II code sets and append required modifiers accurately based on specific payer fee schedule constraints.
5. Same-or-Similar Equipment Overlaps
Same-or-similar denials occur when a patient is billed for DME that duplicates an item Medicare already covered within its Reasonable Useful Lifetime (RUL). Most DME, orthotics, and prosthetics carry a minimum five-year RUL, with limited exceptions such as artificial limbs. Payers reject the new claim if the patient still has a comparable device within that window.
Prevention: Check the patient’s DME history in the applicable Medicare portal before delivery, and where an item may not be covered, follow the payer’s ABN rules so the beneficiary understands potential financial responsibility.
6. Duplicate Claim Submissions
Duplicate claim denials happen when the exact same claim (same patient, provider, date of service, and HCPCS code) is submitted more than once to the same payer. This occurs due to system glitches, resubmitting claims before processing concludes, or accidental entry into the billing software.

Prevention: Implement billing software that scrubs claims for existing submission histories, and wait for electronic remittance advice before submitting corrections.
7. Timely Filing (CO-119 Territory)
Timely filing denials are issued when claims are submitted to the insurer past their strict filing deadline. Medicare allows twelve months from the date of service, but commercial payers often mandate shorter 90 to 180-day windows.
The CO-119 denial code frequently appears when a benefit or filing limit is exceeded, and missing the deadline can forfeit the supplier’s right to reimbursement for that service.
Prevention: Calendar all payer-specific timely filing limits and use your clearinghouse’s automated daily reconciliation process to submit clean claims immediately after dispensing the equipment.
8. Non-Covered Services and Frequency Limits
These denials occur when a billed item violates frequency limits or Medicare’s local and national coverage determinations (LCD/NCD), rendering the service statutorily non-covered.
This happens when a patient receives replacements too soon or exceeds allowed quantities. The CO-96 denial code (non-covered charges) is a classic example indicating a statutorily non-covered service or one that fails coverage criteria.
Prevention: Educate providers on local coverage guidelines and utilize Medicare Coverage Determinations to ensure the patient’s condition and requested frequencies justify medical necessity before placing orders.
Stop Denials at Intake, Not After the Fact
Every denial above is really a documentation problem that slipped through at intake. Fixing it after the fact means rework, delays, and staff hours you can’t get back. Catching it when the order arrives is faster and cheaper, and it’s where CompliantRx works: an AI platform that reviews incoming documentation against the rules before a claim is ever built.
Waiting to catch documentation errors after submission raises your cost-per-order. When you chase denials, you face:
- Delayed Cash Flow: Reworking rejected claims stalls revenue and extends A/R days.
- Resource Drain: Staff spends hours on low-value rework rather than patient intake.
- Audit Risks: Missing signatures or outdated addendums trigger severe penalties.
Prevention requires identifying errors at intake rather than waiting for an explanation of benefits. A compliance-first infrastructure relies on:
- Automated Eligibility Checks: Verifying coverage and prior authorization before delivery.
- Pre-Submission Scrubbing: Reviewing every code and modifier against payer-specific rules.
- Documentation Standardization: Ensuring physician notes match local coverage determinations.
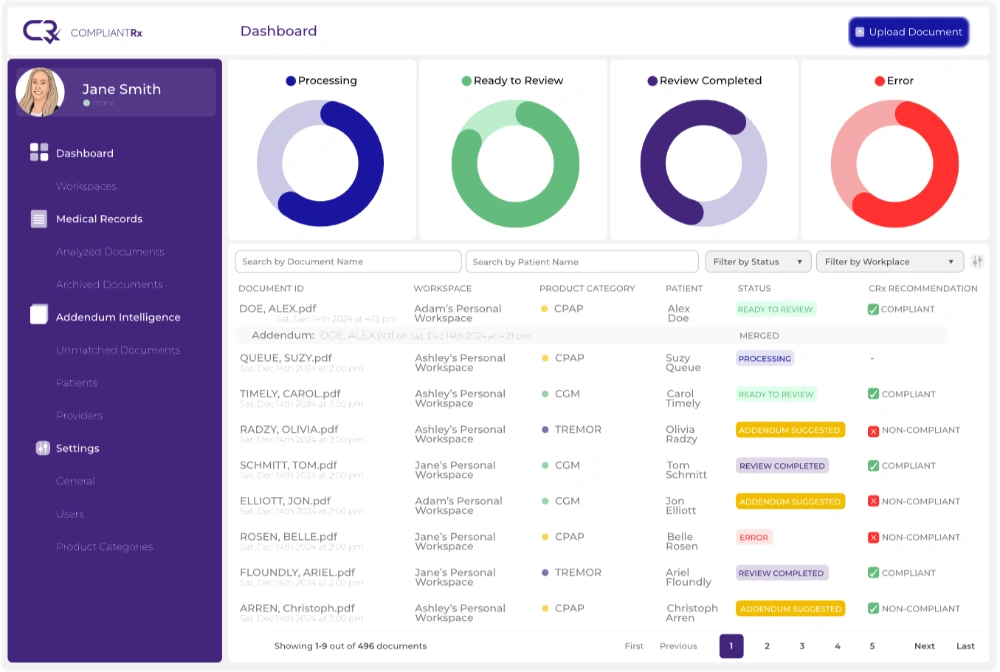
CompliantRx is an AI-powered intake and compliance platform built by a DME operator, for DME providers. It works at the front of your workflow, when the order first arrives:
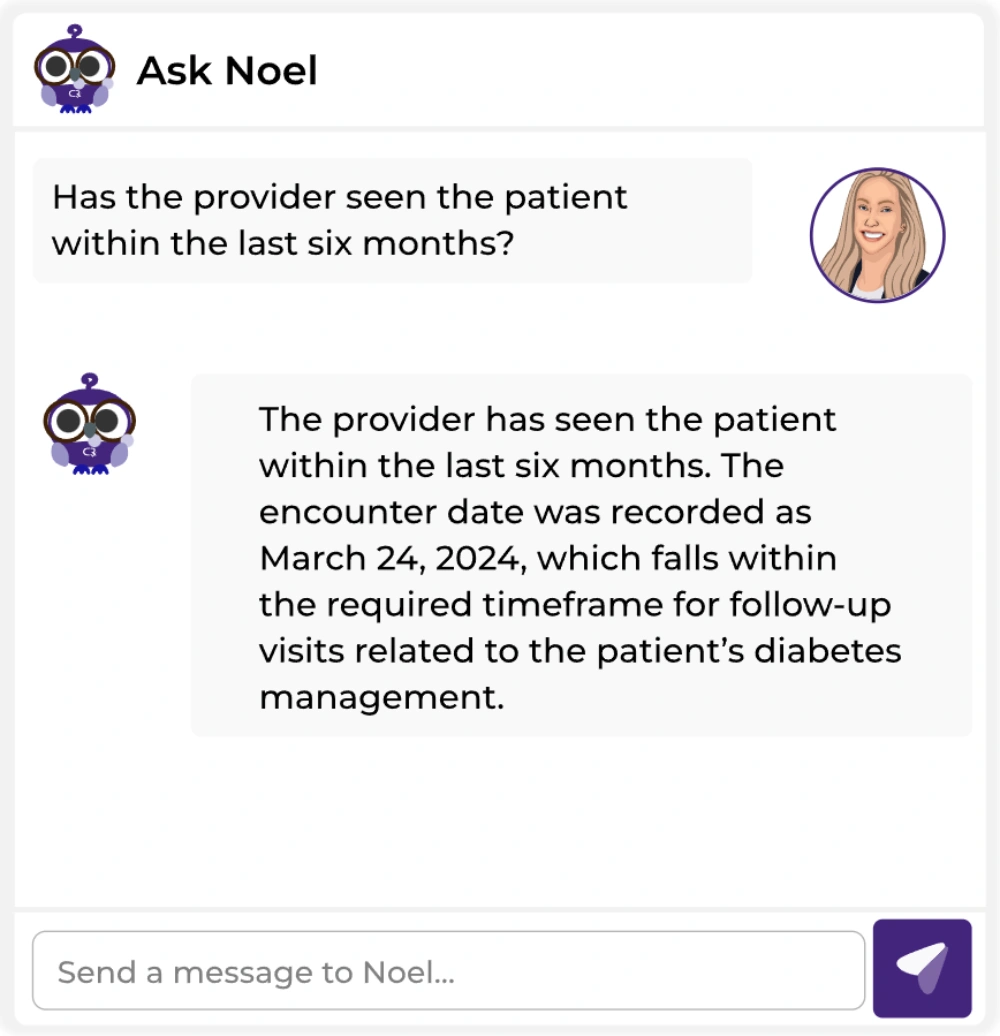
- AI Medical Record Review: Scans incoming documentation against payer- and product-specific rules and flags anything missing before a claim is built.
- Intelligent Data Extraction: Pulls patient and physician details straight from faxes and referrals, reducing manual data entry.
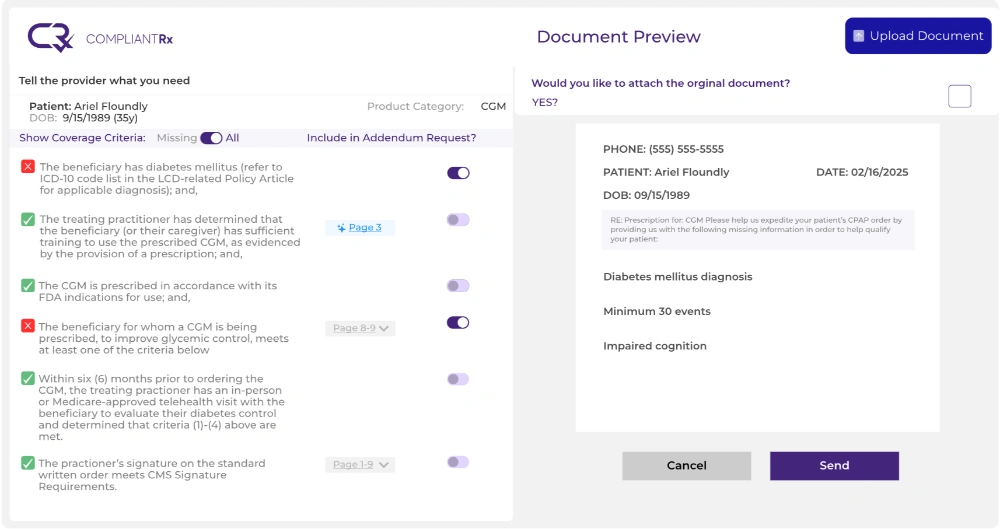
- Addendum Intelligence: Auto-generates the corrective addendum to send back to the provider for anything that’s missing.
- Bi-directional integration: Connects with systems of record like Brightree and NikoHealth without an IT overhaul.
The result is a complete, compliant, ready-to-ship record at the end of intake, so your team spends less time on rework and stays audit-ready.
Key Takeaways – Prevent DME Denials Before They Happen
Every common denial in medical billing on this list is preventable at intake. By verifying eligibility, securing prior authorizations, and completing documentation before the claim goes out, you protect your cash flow and free up your team.
CompliantRx catches these gaps when the order arrives, not after it’s denied. Schedule a demo to see how it fits your intake workflow.
FAQs
Reviewing these frequently asked questions helps clarify any remaining details about a common denial in medical billing.
1. Are commercial payer timely filing limits uniform across the board?
Commercial payers set their own strict filing deadlines, which often differ significantly from standard Medicare windows. Suppliers must verify each payer’s specific timeframes during the intake process to avoid permanent forfeitures.
2. How often should billing teams update their HCPCS code sets?
CMS publishes HCPCS Level II update files quarterly (January, April, July, and October), though the main DME coding changes take effect in January and July. Review each release and update your system before the effective date, since claims with outdated codes can be rejected.
3. Can a missing modifier cause a claim to be rejected entirely?
Omitting a required modifier often makes the claim unprocessable by the payer’s automated system. The system cannot determine the correct reimbursement without knowing if the item was rented or purchased.
4. Why is proof of delivery so heavily scrutinized by auditors?
Auditors use proof of delivery to confirm the supplier actually provided the equipment before billing the payer. Missing signatures or undated documents create compliance gaps that can invalidate the claim.



{kind=link}
{kind=link}
{kind=link}